
Uttara Kannada/Shivamogga/Bengaluru: About 3 km northeast of the Jog falls in Karnataka’s lush Uttar Kannada district lies the quiet hamlet of Jiddi, home to about 800 families, mainly farmers growing arecanut, coconut and pepper.
On one side of Jiddi’s main street stretches a banner celebrating the inauguration of the Ram temple in Ayodhya. Barely visible on the other side is a nondescript poster about KFD, or Kyasanur Forest Disease, a potentially fatal viral illness that causes fever, low blood pressure and internal bleeding, KFD is endemic to this forested region.
In the third week of January 2024, local farmer Jayachandra (name changed) returned home early from his arecanut farm, unusually tired.
The next day, in a febrile state, he visited the local primary health centre (PHC) at Korlakkai, 2 km away. Even as a worried Jayachandra, 38, waited for laboratory test reports on a blood sample, his 54-year-old mother developed a fever. Jayachandra drove them both to Siddapura taluka hospital, 18 km away, where they were admitted.
The state’s first KFD death of 2024 had been recorded in the neighbouring district of Shivamogga. Another positive case had been identified at the same hospital where Jayachandra and his mother were eventually treated for 11 days with intravenous drips and fever medication.

In early March, back at his home in Jiddi, Jayachandra said he knew nothing about KFD until he was diagnosed. “It was never there in my village.”
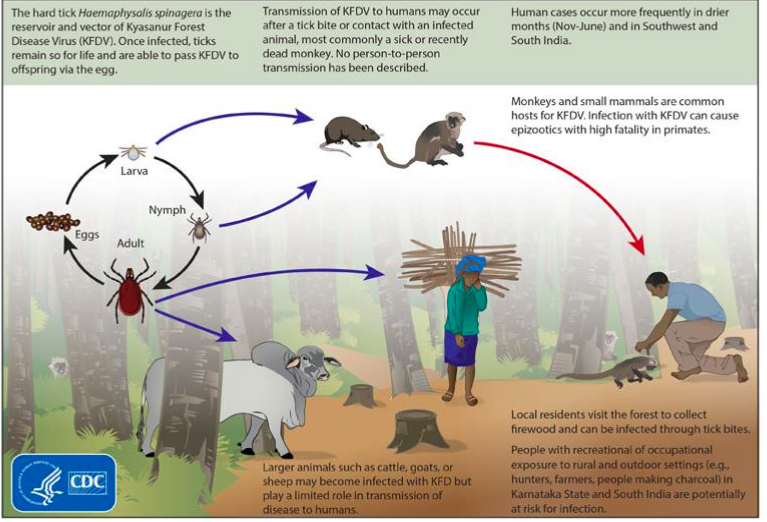
A highly infectious tick-borne disease affecting humans and monkeys, KFD is caused by the Kyasanur Forest Disease virus (KFDV), a flavivirus belonging to the same family of viruses that cause dengue, Zika and yellow fever. The virus is transmitted when ticks carrying the virus bite humans or monkeys.
Until 2012, KFD cases were restricted to five districts in Karnataka—Shivamogga, Uttara Kannada, Udupi, Dakshin Kannada and Chikmagalur. In more recent years, against a backdrop of extensive deforestation, land use change and changing climate conditions, cases have emerged in other Western Ghats states including Maharashtra, Goa, Tamil Nadu and Kerala.
Scientists have linked habitat fragmentation and deforestation to the emergence of KFD cases in other states. N S Prashanth, a medical doctor and director of Institute of Public Health in Bengaluru, said that rapid changes in land use in forests may cause an outbreak of disease, including projects such as roads or railway lines cutting through forests.
“In the Western Ghats, we suspect that new niches are being opened up by macroeconomic shifts,” Prashanth said.
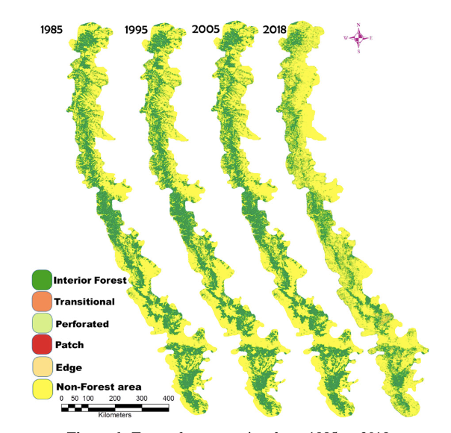
Denuding of the forest cover contributes to changes in the population dynamics of wildlife that are hosts of vector ticks, and between 1985 and 2018, the Western Ghats, which run 1,600 km along India’s western coast, lost 12% of interior (contiguous) forest cover to monoculture plantations of arecanut, acacia, eucalyptus, and to infrastructure projects cutting through once-undisturbed, old-growth forests.
Article 14 has reported (here, here and here) that mamy of these developments violate forest and conservation laws.
In Kerala, the first reported human case was in 2013. The state’s Wayanad district saw a large outbreak in 2015 with 184 cases and nine deaths. Sindhudurg district in Maharashtra witnessed 456 cases in 2016, and 462 KFD cases were reported in Goa between 2015 and 2018.
Marginalised Forest-Dwellers Vulnerable
Sixteen tick species are associated with KFD, with two, Haemaphysalis spinigera and Haemaphysalis turturis, known to be the main vectors. It is a zoonotic disease, like Covid-19. However, there is no recorded human to human transmission. Researchers estimate that India had about 9,000 cases of KFD between 1957 and 2017 .
Bonnet macaques and langurs are highly susceptible to the virus, leading to the disease's nickname 'Monkey Fever'.
In the 1970s, Karnataka was estimated to have the largest bonnet macaque population in south India. Between 1957 and 2020, at least 3,314 monkey deaths have been attributed to KFD. Small rodents and cattle are reservoirs of infected ticks too, though they do not develop symptoms.

Smallholder farmers such as Jayachandra, plantation workers and people dependent on forest resources for livelihoods are particularly vulnerable. The disease has been called a ‘neglected disease of poverty’ due to lack of awareness and poor access to diagnostic services.
Darshan Narayanswamy, a researcher at the Ashoka Trust for Research in Ecology and Environment (ATREE), Bengaluru, said most patients were from lower-socio economic backgrounds. “They do not have much nutritional food, so they become infected very soon,” he said.
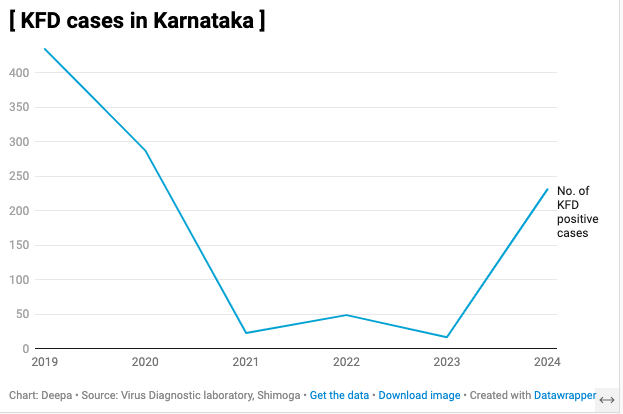
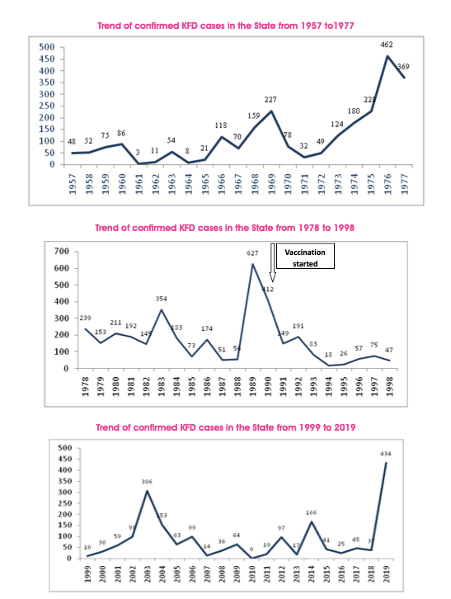
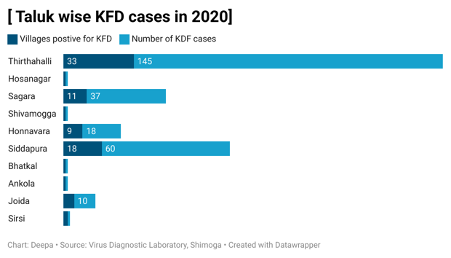
KFD affects approximately 500 persons annually in India with outbreaks occurring during the dry months, between November and March. Since the first case was reported in the Kyasanur forest of Shivamogga district in 1957, there have been sporadic outbreaks in Karnataka recorded in 1976, 1977, 1983, 1989, 1990, 2003, 2019 and now 2024. By 31 March 2024, Karnataka reported 231 cases of KFD and 12 deaths, including that of a seven- year old girl from Jiddi.
Deforestation, Climate Change & KFD

The Western Ghats are a mountain range older than the Himalayas, dating back 150 million years to the Jurassic age, inscribed in 2012 on a World Heritage List and described as one of the world’s eight “hottest hotspots” of biological diversity.
The Western Ghats influence the south-west monsoon, and feed three of India’s seven biggest rivers, supplying water to much of the Indian peninsula, home to about a fourth of the country's population.
Data from the Landsat satellite suggest that in Shivamogga district, ground zero of repeated KFD outbreaks, forests declined 7.6%; farms grew 4.8% and urban areas grew 4.6% between 2010 and 2020.
K P Sripal, advocate and member of KFD Janajagruthi Okkoota in Shivamogga, is fighting a case against the state government to stop acacia plantations, a non-native species. These plantations increased the temperature of the area, he said. “The loss of natural forests is causing wild animals to come to residential areas,” said Sripal.
A statewide survey between 2002 and 2007 showed that groups of bonnet macaques, five to 75 in each, were largest near human habitations including temples, roadsides and farms where food was easily available, and where chances of monkey-human encounters were high.
Narayanaswamy from ATREE said, “Unseasonal rains and increasing temperature also affect the outbreak of the disease.” High temperatures of 28°C to 30°C from December to May are associated with high tick density.
The MonkeyFeverRisk project by scientists who analysed factors behind the spread of KFD cases studied patterns of human outbreaks from 2014 to 2020. They matched cases with land use change patterns from satellite data, climate and health systems data.
This initiative found that human outbreaks of KFD were more likely in areas that had a high percentage of moist evergreen forests, forest fragmentation due to paddy, plantations and high densities of indigenous cattle.
Bethan Purse, an ecologist at the UK Centre for Ecology and Hydrology, and also principal investigator of the project, said land use changes could make the habitat conducive to small mammals that amplify transmission of the KFD virus.
Social drivers also play a role. Stefanie Schafer, a vector ecologist with the team, said workers go into cashew plantations for harvest work when KFD virus activity is also peaking.
“Other activities, such as gathering dry leaves from the forest floor to make manure bring the ticks close to human and livestock habitation, and increase risk of KFD,” Schafer said.

These factors may open up the possibility of pathogens expanding their range of hosts and adapting to new niches, making it challenging to predict and control outbreaks.
A Control Strategy Without A Vaccine
Since 1990, a KFD vaccine made from the virus treated with a chemical, formalin, to inactivate it, was administered, but not exhaustively.

Surveys conducted on 343,256 individuals eligible for KFD vaccination found that 52% did not receive any vaccine. The effectiveness among those who received it was only 62.4%.
In 2023, the vaccine was withdrawn citing ineffectiveness and lack of approval from the World Health Organisation.
Without a vaccine, the only preventive measure currently is a tick repellent oil, distributed by accredited social health activist (ASHA ) workers.
“Villagers are told to apply the oil before going to the forest or plantations,” said Narayanswamy from ATREE. Full clothing is also recommended, which is not the normal practice. They are also told to wash their clothes in hot water upon returning, he said.
In order to develop a predictive tool to prepare for likely outbreaks, the Monkey Fever Risk Team in collaboration with the Karnataka state department of health and family welfare services developed spatial risk maps in 2020, based on the relationship between deforestation and human outbreaks.
“These risk maps can identify potential hotspots of risk that are outside the known distribution of the outbreaks,” said Purse. The maps were used to target vaccination and surveillance in new risk areas.
Harshavardhan, medical doctor and deputy director at the Virus Diagnostic Laboratory (VDL) in Shivamogga, said his predecessor had undertaken the creation of spatial maps as a tool, but its use slowed due to Covid-19. “We plan to upload the surveillance data from mid-April onwards and it will be helpful from next year onwards,” he said.
A ‘One Health’ Approach
Early detection of and surveillance for zoonotic diseases such as KFD needs a one health approach that holistically considers the connected health of humans, domestic and wild animals, plants and the environment.
Prashanth NS said for KFD this would mean surveillance of humans, wildlife, cattle and domestic animals. “Currently, there is no robust wildlife disease surveillance,” he said. A timely data reporting and sharing system was also missing, he said.
Cattle could be treated with an acaricide (pesticide for ticks), said Purse, but there is currently no government program to treat cattle with anti-tick medications. This is done only at farmers’ requests, said Shivanand Yali, a veterinarian, from the state animal health department.
The union government’s department of animal husbandry and dairying (DAHD) launched a ‘One Health’ pilot project in 2022 in Karnataka, to form the basis for development of a One Health Framework for India. Article 14 sent emails to the DAHD regarding the outcomes of the pilot, but these remained unanswered.
An official from the National One Health Mission, who did not want to be named, said India needs disease-specific solutions as well as commonalities for zoonotic diseases.
Experts cited the lack of coordination among animal, human and wildlife departments, and lack of leadership to steer implementation. “There should be a clear one health action plan,” said NS Prashanth, “identifying which sector will take the lead and who will be the convener for meetings.”
A Neglected Disease Affecting Forest Villages
Kiran Kumar, medical doctor, at the Korlakai PHC, who handles cases from Jiddi and other nearby villages, said most doctors are unaware of KFD and normally don’t test for it. “They think of testing for KFD only retrospectively, after three to four human deaths,” he said.
Stigma also drives patients to private clinics, away from PHCs.Jiddi residents said they were shunned by people from other villages, including their own relatives, perhaps because the disease is believed to be transmitted from monkeys.
Testing for KFD is done only in government hospitals or at Shivamogga’s VDL. Blood samples of suspected cases from a PHC may take up to two days to arrive at VDL.
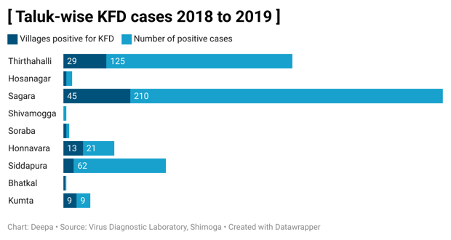
Around 25 km south-west of Jiddi lies the village of Aralagodu in Sagar taluka, close to the Sharavathi wildlife reserve. In 2018-19, Aralagodu was the epicentre of a KFD outbreak. No cases were reported in 2024, but timely diagnosis remains a hurdle.
K Hegde, the sole doctor at the local PHC, said the very remote Aralagodu does not have a bus service. An ASHA worker or nurse has to take the sample by a private vehicle to Sagar, 40 km away. The next morning, the samples then travel another 70 km to VDL. Results may thus be available only three-four days after testing.

In 2018-19, even this routine was not established. Shivaraj, an Aralagodu resident who was active in highlighting the KFD cases to the media, said it was after the first death occurred in December 2018 that awareness emerged. “Only then did we come to know of such a disease,” he said. “One month later, the government started administering the KFD vaccine.”
It was too little, too late. By the end of March 2019, this tiny hamlet with a population of about 2,000 had recorded 165 cases and 22 deaths. Residents faced social stigma and economic hardship. “People were scared of going to the hospital,” Shivaraj said “Many gave away their cows, and left for 2 to 3 months.”
Radha, a 43-year-old mother of three who did not want to give her full name, lost her husband, a daily wage plantation worker, to KFD as he was afraid to go to the hospital. Although the government provided Rs 2 lakh as compensation, it wasn’t enough. Her son had to drop out of school after Class 8 to add to the household income.
Prashanth explained that some of these communities may not have confidence in government programmes. “There's a lot of health literacy issues,” he said, “but there's also system failure in reaching out to these communities in a trustful manner.”
Inadequate Management And Surveillance
After the 2019 outbreak, advocate KP Sripal filed a writ petition against the government of Karnataka for failure to prevent the spread of KFD. Apart from vaccines and better diagnosis, the petition sought directions on awareness and precautionary measures in areas prone to the disease.
Ravindra K B, state medical health officer at the KFD field station in Sagar, said since the 2019 outbreak, surveillance has been undertaken regularly. He said ASHA workers from the respective PHC go house to house in a 5-km radius from a hotspot. “If they find a person with fever, they are directed to the PHC for a blood test,” he said.
Ticks are surveyed in forest areas and along paths frequented by villagers, he said, but residents of Jiddi and Aralagodu said they were not aware of tick surveillance until after the outbreak.
When a monkey's death is reported, a team inspects the body, said Ravindra. If fresh, organs are collected and sent for autopsy at the National Institute of Virology in Pune. If decomposed, the body is burned, and the area is sprayed with the insecticide to kill the ticks, he added.
A study published in PLOS Neglected Tropical Diseases journal in 2021 on KFD management practices in India noted that burning monkey carcasses and spraying pesticide are likely to be ineffective as infected ticks can be found in wider areas.
Purse said their modeling work showed that small mammals such as shrews, mice and rats, currently not included in disease surveillance, are more important in amplifying the transmission of KFD than monkeys.
The virus is transmitted when nymphs, adolescent-stage ticks active from November to May, bite humans. Symptoms including fever, headache and vomiting emerge three to eight days later. Most patients recover in one or two weeks, but some experience a severe second phase marked by neurological problems and fever. This phase lasts longer, and may be fatal.
A week after returning from the hospital, Jayachandra experienced a relapse. He was treated again, but recovery was slow. Aching joints still hamper his movements, and an extreme fatigue sets in quickly.
Early summer temperatures in 2024 were 2 to 3o C above normal in Karnataka. Jayachandra is no longer able to provide food for his family. “I can't bear the sun, so I can't work on the farm,” he said. “The heat is increasing every year.”
(Deepa Padmanaban is a freelance journalist based in Bengaluru.)
Editor’s note: The story was produced with the support of a One Health grant from Internews’ Earth Journalism Network. The author is a freelance journalist and consultant (media and outreach) at the Centre for Wildlife Studies. She declares that there is no conflict of interest between these two roles and that she has not interviewed colleagues or cited research funded by the Centre for Wildlife Studies for this report.
Get exclusive access to new databases, expert analyses, weekly newsletters, book excerpts and new ideas on democracy, law and society in India. Subscribe to Article 14.