Delhi: Two new studies have confirmed anecdotal evidence and data from older studies: that Adivasis, Dalits and Muslims live shorter lives than upper-caste Hindus—and even other backward Hindu castes—with the disparity between upper-caste Hindus and Muslims widening over the last two decades.
Compared to upper caste Hindus and other backward castes (OBCs), Adivasis die four years earlier, Dalits three years earlier and Muslims a year earlier, according to the first new study, published in March 2022 in the Proceedings of National Academy of Sciences (PNAS), a global scientific journal.
The second new study, published in April 2022 by two US and Indian researchers in the Population and Development Review, a global journal, reported that the Muslim life-expectancy gap with upper-caste Hindus had worsened from marginal—2.1 years in women and 0.3 years in men in 1997-2000—to about 2.8 years in women and 2.6 years in men in 2013-16.
The differences between the life expectancy of higher-caste Hindus and the life expectancies of Adivasis and Dalits are comparable to the Black–White gap in the US in terms of “absolute magnitude”, said the PNAS study, released in March 2022 and conducted by three researchers from India and US.
The researchers of the PNAS study found the reasons for the disparities were not wealth alone, since economic status explained less than half the life-expectancy gap, which could not be accounted for even by environmental factors and urban-rural differences.
The researchers said further research on causes of death, segregation, behaviours, and risk factors, such as occupational exposures in the social groups, may help understand the disparities in mortality and life expectancy.
Marginalised social groups in India—Dalits, Adivasis and Muslims—compose a population of over 450 million, greater than that of the United States. Each of these groups are among the largest marginalised social groups in the world. The findings of the latest study are in line with other studies and data (here and here) that point to similar disadvantages for these groups.
Life expectancy is among the most important human development and health indicators and provides a third weightage in calculating the United Nations’ Human Development Index. These kinds of disaggregated data by caste and religion are important to understand what experts called the “lived experiences” of various social groups in India.
But these data were not available before because the Vital registration system that records all births and deaths in India is incomplete (completeness of death registration in India ranges from 58% in 2000 to 81% in 2018) and India relies on the national Sample Registration System, a set of national data, for mortality estimates but these do not aggregate life expectancy by caste or religion.
Why India Needs To Confront Social Inequality
The life expectancy study published in the PNAS used India’s Annual Health Survey (AHS), a household survey of data garnered when surveyors visited over 4 million households in nine poor states between 2010 to 2011. These states were Assam, Bihar, Chhattisgarh, Jharkhand, Madhya Pradesh, Odisha, Rajasthan, Uttar Pradesh and Uttarakhand. Together, these states represent almost half of India’s population.
The study published in the Population and Development Review, using data published in two rounds of the National Family Health Survey (1998-99 and 2015-16), showed that scheduled castes (SCs) and scheduled tribes (STs) had lower life expectancies than higher castes.
The difference between SCs and STs and upper-caste Hindus was 4.2 to 4.4 years for women and 6.1 to 7 years for men. The study also found that while Muslims had a modest life expectancy disadvantage (2.1 years in women and 0.3 years in men) compared to high castes between 1997 to 2000, this disadvantage has grown substantially (2.8 years in women and 2.6 years in men ) over the last 20 years.
The studies highlight the “need to confront social inequality directly, rather than hoping that economic growth will tackle health inequalities,” said Aashish Gupta, David E. Bell fellow, Harvard University, and a research fellow at the Research Institute for Compassionate Economics (known as r.i.c.e), and a co-author of both the studies.
The studies confirm the suspicions of public health experts that disparities between social groups have resulted in differences in health outcomes.
“It may seem that it is just one year or two years difference between the social groups,” said Aqsa Shaikh, associate professor of community medicine at the Hamdard Institute of Medical Sciences and Research, New Delhi who is not involved in the studies. “But it means a lot in terms of health outcomes because increasing just one year of life expectancy requires a lot of effort, so a decrease of one year is also significant,” she said.
Adivasi Women & Men Live Shortest Lives
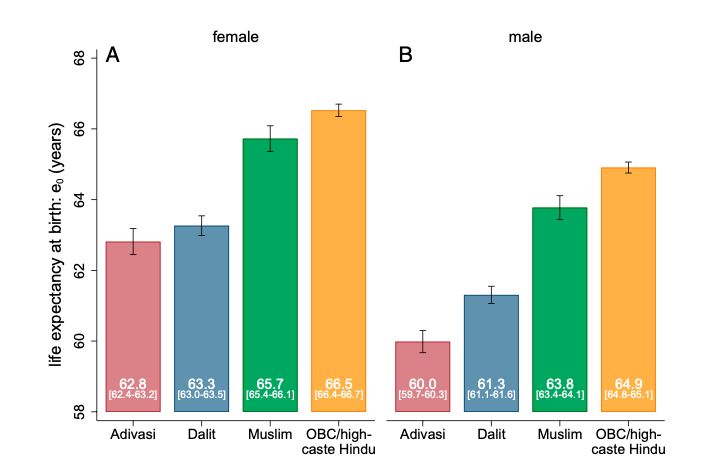
The PNAS study showed that life expectancy at birth was highest for higher caste/ OBC Hindu women at 66.5 years, followed by Muslim women at 65.7 years, Dalit women at 63.3 years and Adivasi women at 62.8 years.
The researchers do not have separate estimates for higher castes and OBCs because the AHS does not provide them separately. They assumed that the life expectancy for OBC and higher castes was lower than the life expectancy for higher castes alone, since OBCs have a higher population but are more marginalised than higher castes.
Among men, the highest life expectancy was for higher caste/ OBC Hindu men at 64.9 years, Muslim men at 63.8 years, Dalit men at 61.3 years and Adivasi men at 60 years.
Researchers pointed that Muslims have a lower disadvantage in life expectancy compared to other marginalised social groups because of a variety of factors—lower exposure to open defecation among Muslim children, lower rates of cervical cancers among Muslim women, lower consumption of alcohol and lower incidence of suicide.
Exposure to open defecation is a key determinant of human capital. Germs in faeces cause diarrhoea and other diseases that harm children’s growth and mother’s health. It is linked to India’s higher infant mortality, high anaemic population and its high number of underweight women. Recent evidence proves exposure to open defecation is the main reason why Indians are shorter than those living in sub-Saharan Africa despite being richer.
The life expectancy of Dalits was lowest in Uttar Pradesh and that of Adivasis was lowest in Madhya Pradesh.
Disparities among different groups are low in Uttar Pradesh, which also has the lowest life expectancy among all nine Indian states. This could be because of poor environmental health and healthcare provision, noted the researchers.
The states with the most disparity—more than five years of difference in life expectancy between OBC/high-caste Hindus and a marginalised social group— include Uttarakhand, Jharkhand, Odisha, Chhattisgarh and Madhya Pradesh.
Why Wealth Does Not Bring Parity In Life Expectancy
Can wealth explain the differences between the social groups? Not quite.
The researchers in PNAS study found that Adivasis and Dalits have lower life expectancies than OBCs and high-caste Hindus across wealth categories. Wealth explains only half of the gap between the groups, as we said. Neither do rural or urban or environmental factors fully explain the difference in life expectancy between the castes.
That is because other than wealth, a number of factors impact health outcomes, such as access to clean water, nutritious food, access to good housing and employment, said experts.
“You can’t be healthy when you are focussed on surviving,” said Kiran Kumbhar, physician and PhD candidate studying the history of medicine at Harvard University and not associated with both the studies. “Stress that comes with living as an underprivileged and poor takes a toll on people’s physical health.”
Healthcare providers display a bias against Muslims and SCs and STs, affecting their access—a third of Muslims, over 20% of Dalits and Adivasis, and 30% of all respondents reported being discriminated against on grounds of religion, caste or because of illness or health conditions in hospitals or by healthcare professionals, noted a November 2021 Oxfam India report.
In 20 Years, Life expectancy Improved But Differences Remain
In the Population and Development Review paper, life expectancy was estimated for all social groups at birth, at 15 years of age and at 60 years in 1997-2000 and 2013-2016.
The researchers found that while life expectancy improved over the two decades to 2016 in all groups, there were large differences. For example, in 2013-2016, compared to higher castes, life expectancy for SCs was 4.4 years lower and 6.1 years lower for men; among STs, it was 4.2 years lower in women and seven years in men.
The absolute difference in life expectancy increased among SC and higher caste men between 2013 and 2016 (6.1 years) as compared to 1997-2000 (4.6 years). By comparison to the US, differences in life expectancy between Blacks and Whites in 2015 (3.5 years) were half of that in 2000 (7 years).
The studies disabuse the notion that economic progress has reduced disparities.
“I think the discourse is that India has achieved economic progress and things are going in the right direction but what is forgotten is that most of the benefits of whatever changes have taken place have been concentrated or usurped by people from privileged backgrounds,” said Kumbhar.
“Considering that the so-called middle class in India is not more than 10-15 % of the population, it is clear that the country's economic progress over the past 30 years has hardly brought any substantial improvements in the health and living standards of most Indians,” said Kumbhar.
Muslim Life-Expectancy Advantage Is Diminishing
For years, researchers have discussed the ‘Muslim Mortality Paradox’, data that showed Muslim infants had a lower chance of dying before their first year, as compared to Hindu infants, despite economic disadvantages.
Driving this paradox was the higher use of toilets by Muslims (here and here), providing Muslim children a disease-free environment to grow-up.
Predictably, the difference in life expectancy of Muslims and high-caste Hindus was the smallest: between 1997 and 2000, the difference in life expectancy at birth among Muslim and high-caste Hindus was 2.1 years among women and 0.3 years for men. This difference was smallest at birth and increased with age.
By 2013-16, the difference in life expectancy at birth between Muslims and Hindus had increased to 2.8 years in women and 2.6 years in men and widened with age.
The Unaddressed Disparities In Health Policy
The authors of the Population and Development Review study noted their findings suggested that more attention be paid to India’s marginalised communities, who continue to face mortality disadvantages despite rapid economic growth.
The researchers also stressed that efforts need to move beyond a focus on child health to understand the sources and ways to reduce disparities among adults globally. Population health interventions need to challenge social disadvantage because economic progress may not be enough.
“Unfortunately, health policy in India and globally largely ignores exploitation, violence, and discrimination rooted in social inequality,” said the PNAS study. “This study justifies further action on social disparities in health within India and advances the global conversation addressing inequalities based on race, ethnicity, indigenous identity, caste, and religion.”
In order to improve health outcomes, it is important to have baseline data and to accept that the problem exists, said Shaikh. Only then can solutions be found, such as those that have worked elsewhere. An example, she said, was affirmative action in the US, which increased the number of Black Americians in the healthcare system, focussing specifically on where African-Americans were located.
(Swagata Yadavar is an award-winning health writer based in New Delhi.)